by John J. Case, Kimberly P. Ellis
As presented at the 2019 Winter Simulation Conference
Abstract
In collaboration with the leadership team at a major metropolitan hospital in the United States, the research team develops alternatives to improve the hospital’s discharge system to increase the availability of bed space for new patients. Following a multi-day site visit, we utilized service time data to develop a discrete event simulation (DES) model to evaluate discharge improvement strategies, assuming fixed capacity. We found that a Percent-by-Time discharge strategy improved the hospital’s patient holding time by a minimum of 24% if implemented in all service areas. This zero-cost strategy requires no increases to hospital resources and can improve patient flow and timely access to healthcare in highly utilized hospitals.
Introduction
In 2017, a major metropolitan hospital experienced average bed occupation of 93% and periodic unavailability of bed space for new in-takes due to an average intake of 1PM and an average discharge of 3PM. The hospital’s leadership desired to improve the discharge time of day in order to alleviate the scarcity of available bed space for new patient intakes. The authors visited the hospital where we observed patient flow processes, interviewed doctors, nurse practitioners, nurses, social workers, case managers, and housekeeping and administrative staff in multiple surgical and medicinal hospital services.
Methodology
The hospital had many different service areas, each with their own discharge policies, timelines, and staffing plans. We chose to simulate Hospital Medicine and Internal Medicine because these had the latest mean discharge time of day and the highest volumes of patient flow, indicating greater room for improvement and impact on the hospital as a whole. We also modeled Colorectal Surgery, which had the earliest hospital-wide mean discharge time of day and would provide a lower bound on anticipated improvements. We used hospital-provided empirical patient flow data, conducted data analysis in R, and modeled the chosen services with SIMIO® DES software.
Assuming that bed space and care provider capacity is fixed, we simulated reducing the discharge process time by 50%, writing discharge orders earlier in the day (by 1, 2, and 3 hours earlier), and a Percentby- Time strategy, adapted from the novel n-by-T strategy described by Bertsch (2014).
Results
The Percent-by-Time strategy proves to be the most efficient method to reduce patient holding without needing to overhaul the scheduling and staffing in the different hospital services. The DES results are summarized in Figure 1 for Hospital Medicine, Internal Medicine, and Colorectal Surgery.
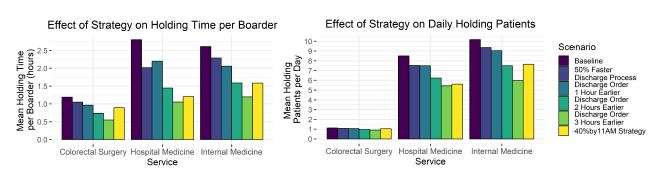
Figure 1: Simulation results.
The simulation results showed that the most effective technique to reduce patient holding was writing discharge orders three hours earlier, however it is not an efficient or flexible strategy and cannot be widely implemented due to service-specific constraints. We recommend the Percent-by-Time and these methods:
- Physicians should begin rounding by 7 AM and prioritize seeing patients by potential current-day discharges first, sickest patients second, and then in descending order of acuity.
- Discharge huddles should primarily focus on future discharges, rather than current-day discharges.
- Nurses should select patients for early discharge based on the number and length of tasks required to discharge those patients, prioritizing the patients with the shortest total time requirements first.
- The Percent-by-Time strategy should be executed by Admit-Discharge-Transfer (ADT) nurses.
The Percent-by-Time strategy is an adaptation of the shortest processing time sequencing heuristic and seeks to free up bed space earlier in the day by identifying and discharging the “fast” patients first, then proceeding as usual for the remaining patients. As shown below in Figure 2, shifting 40% of the discharge time distribution to occur before 11AM, the hospital avoids much of the holding that begins in the late morning each day. Interviewed care providers thought that prioritizing 40% “fast” patients was achievable.
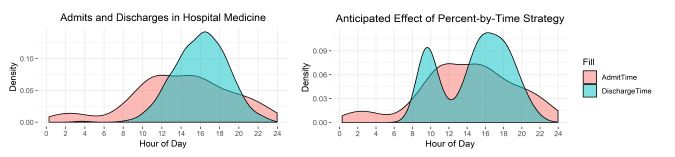
Figure 2: Empirical and 40%-by-11AM admits and discharges by time in hospital medicine.
With this strategy, Hospital and Internal Medicine have an expected percent decrease in patient holding times by 57% and 39% respectively, which is likely an upper bound for other services. Colorectal Surgery’s expected percent decrease in patient holding time (24%) will likely be the lower bound for the hospital, if the 40%-by-11AM strategy is fully implemented hospital-wide. The zero-cost Percent-by-Time strategy can be extended to highly utilized hospitals. For hospitals that lack the ability to increase capacity, the Percent-by-Time is an effective strategy to decrease patient holding and increase timely access to care.